Beyond Efficacy: Why Primary Research Should Shape Formulation, Route-of-Administration and Trade Dress Decisions
By Noah Pines
When an investigational new medication produces exceptional efficacy data, it is tempting to assume the market will reward it accordingly. Yet in practice, uptake depends not just on clinical outcomes but also on how well the treatment fits into the rhythms of real lives.
Adherence is shaped as much by the formulation and administration experience as by the molecule itself. That is why robust primary research, qualitative and quantitative, must guide formulation and route-of-administration decisions. And that's why teams need to start thinking about this early on in the new product development cycle.
The Adherence Reality Check
Evidence consistently shows that reduced dosing frequency correlates with higher adherence. A randomized simulation comparing twice-daily (BID) versus three times daily (TID) dosing demonstrated that TID participants had significantly more early, late, and extra doses, while BID participants were more likely to maintain correct daily adherence by day. Similarly, meta-analyses have confirmed that once-daily regimens improve adherence, compliance, and persistence relative to more complex dosing schedules.
But frequency is only one axis. Cross-sectional research highlights that patients’ preferences extend to the physical form -- small tablets, pleasant-tasting solutions, or easy-to-handle capsules -- and these preferences strongly influence medication persistency (i.e., compliance over time). Tablet size, taste, and even color can determine acceptance. Oral routes dominate in preference, but within pediatrics, sachets, syrups, and oral solutions often outperform tablets for acceptability, especially when caregivers are responsible for administration.
Designing Research: Who to Talk To
To help inform formulation and administration decisions that will endure commercially, a multidisciplinary respondent mix often is ideal. We recommend striving to include all of the relevant stakeholders including those who will be the direct, end-users, but also those who will prescribe, inform, educate and dispense.
Patients for real-world usability and trade-offs.
Parental caregivers for pediatric or dependent populations.
Caregivers of elderly patients
Physicians and advanced practitioners for initiation and prescribing dynamics.
Nurses for training, questions and troubleshooting.
Pharmacists for substitution, abandonment, and everyday administration queries.
Each group sees different friction points. Together, they offer a 360° view of where adherence breaks down and how experience design can pre-empt it.
Methodological Considerations
Designing primary research to inform formulation and route-of-administration decisions requires a balance of rigor and pragmatism. Done well, it produces insights that are both human-centered and statistically reliable. Here are some key considerations:
1. Qualitative Research: Building the Friction Map
Qualitative methods are the foundation for understanding the lived experience of taking a medication. They uncover the critical “why's” behind adherence, or non-adherence.
Interview depth and structure: One-on-one interviews (IDIs) allow patients, caregivers, or HCPs to walk through their medication routines in detail. Semi-structured topic guides are best: they provide comparability across respondents while leaving space for unexpected themes to spontaneously emerge.
Contextual methods: Techniques such as diary studies, “day-in-the-life” probes, and device-handling exercises often surface usability challenges that respondents wouldn’t articulate in a standard Q&A format. For pediatrics, diary entries by parents can highlight peak stress points (e.g., before school, bedtime) where medication use is most fragile. Digital ethnography can be effectively employed in this regard.
Sample size guidance: For qualitative research, the aim is not representativeness but saturation: the point at which new interviews no longer yield new themes. In practice, 15–20 patients per segment (e.g., adults vs. caregivers, oral vs. injectable users) often achieves this. When testing multiple device prototypes, adding usability cohorts of 8–10 respondents per round can reveal error patterns quickly.
Output: The deliverable from qualitative work is typically what we call a “friction taxonomy,” which is essentially a structured map of barriers (practical, emotional, contextual) and the attributes that matter most to stakeholders. This taxonomy becomes the raw material for quantitative design.
2. Quantitative Research: Validating and Prioritizing Attributes
Quantitative methods take the rich but anecdotal findings from qualitative work and scale them into the evidence to support decision-making.
Choice modeling: Discrete choice experiments such as conjoint analysis or maxdiff are especially useful here. They force respondents to make trade-offs between competing features, revealing the relative importance of attributes such as dosing frequency, pill size, or injection discomfort.
Sample size and power: Because conjoint models estimate utility scores across multiple attributes, larger samples are essential. For a standard conjoint with ~6–8 attributes and 3–4 levels each, a minimum of 200–300 respondents per major segment (patients, caregivers, HCPs) is advisable. For particularly high-stakes decisions (e.g., green-lighting a new injectable platform), 500+ can provide the robustness needed to simulate market uptake scenarios with confidence.
Segmentation: Include sufficient sample to test for heterogeneity, i.e., disparities between subgroups such as adolescents vs. adults, early vs. late-stage patients, or high- vs. low-adherence cohorts. This often reveals that a single formulation cannot meet all needs, guiding portfolio or lifecycle planning. Indeed, in our experience, we have often identified different segments and age cohorts based upon mode of administration habits and preferences.
Output: Utility scores, importance weights, and market simulations. These allow teams to ask “what if” questions (e.g., “What if we launched a once-weekly sachet with mild taste masking versus a daily tablet?”) and estimate the impact on preference shares.
3. Study Design Practicalities
Stimuli design: Attributes should be grounded in qualitative insights but expressed in plain, patient-friendly language. For example, “needle gauge: 27G” should instead be described as “very thin needle, designed to minimize pain.” We often anchor discussion in TC-specific analogies, e.g., "like an insulin needle."
Mode of research: Digital surveys are efficient, but for sensitive populations (pediatrics, HIV, rare diseases), hybrid approaches, combining in-person interviews, caregiver-assisted surveys, or moderated online tasks, often yield richer data.
Ethical and compliance safeguards: For pediatric research, strict parental consent and age-appropriate communication are essential. Involving adolescents directly can be invaluable, but only when done with protocols that prioritize safety and assent.
Triangulation: Consider layering methods, e.g., following conjoint with a short qualitative debrief to explore the reasoning behind choices, or pairing HCP survey data with observational pharmacy audits.
4. Sequencing for Impact
The most effective programs use a staged approach:
Exploratory qualitative to identify friction points and generate attribute sets.
Pilot conjoint/maxdiff with a smaller sample to refine design.
Full-scale quantitative with robust sample sizes to validate and simulate market impact.
Integration workshops bringing R&D, commercial, and medical teams together to translate findings into target product profiles (TPPs) and development decisions.
Trade Dress: The Color, Shape & Visual Identity of the Pill
Patients remember more than dosing schedules and flavor. They remember how their pills look, how they feel in the hand, how easily they identify them among other meds. Trade dress refers to the visual identity: color, shape, finish, imprint, coating -- elements that are often judged secondary, but which in our experience carry real behavioral impact.
Following are key considerations when testing trade dress, along with what our experience and public examples show.
What Trade Dress Can Do
Recognition and recall: When the pill is visually distinctive (color or shape), patients are more likely to differentiate it from generics, other prescriptions, or supplements. This helps them remember “which pill to take, when.”
Brand equity and preference behavior: A recognizable color or shape can enhance perceived legitimacy or prestige. Some patients ask for a pill by its color (“the purple pill”), which can support adherence and brand awareness.
Consistency and trust: Variability or look-alike generics can confuse patients or reduce perceptions of reliability. A unique appearance that is consistent over time helps build trust.
Public Example: Prilosec / Nexium & the “Purple Pill” Strategy
As industry lore confirms, Prilosec (omeprazole) was long known colloquially as the “purple pill.” When its patent neared expiry, AstraZeneca introduced Nexium (esomeprazole) under a “new, improved purple pill” branding strategy -- essentially preserving the color equity while repositioning the product for its next lifecycle.
It’s a useful business case because it demonstrates how color alone, apart from molecular change, can be part of a brand transition strategy. Even when generics enter, that color identity can remain a point of differentiation.
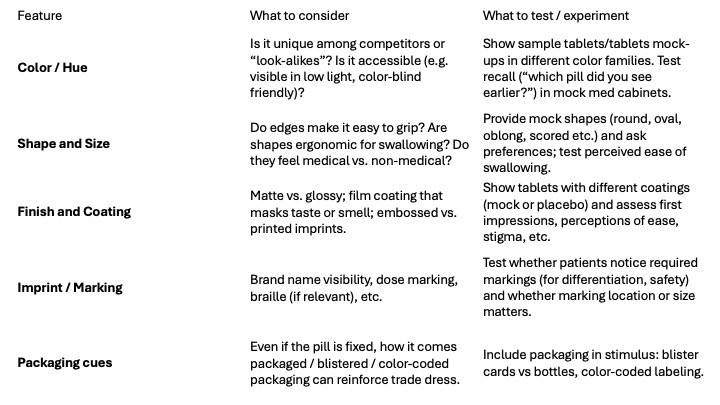
What to Test & How
When running trade dress experiments, these are the levers and methods that tend to reveal the strongest effects:
Experimental Designs & Sample Considerations
Qualitative first: Use small mock-ups or even simple rendered images to explore emotional reactions to different colors/shapes. Use “memory tests” in interviews (“show me what pill you’d reach for first”) or diary/photo elicitation.
Quantitative follow-on: Incorporate trade-dress features into choice experiments (conjoint) along with functional attributes (frequency, dose form, size, etc.) to see how trade dress interacts with other trade-offs.
Segment size: Since trade dress may mean different things to different groups (older vs younger; with vs without visual impairment; chronic vs acute; urban vs rural), ensure adequate subgroup power. For example, 200+ per segment might suffice when trade dress is one of 6–8 attributes; if trade dress ends up being a strategic differentiator, consider oversampling to reduce error bounds.
Salience / priming: Be sure the stimuli are presented in ways that reflect how patients actually encounter pills (in blister packs; among multiple pills; in dim light; with the cap off etc.), not just idealized white background photos.
Why Pediatric Medications Demand Special Attention
Pediatric populations pose unique adherence challenges. Children frequently resist large or bitter-tasting tablets, and parents often struggle with splitting doses, measuring suspensions, or coordinating multiple daily administrations.
Studies confirm that caregivers value smaller, flavored, or liquid formulations, and in some contexts, adolescent patients themselves can provide critical input on which dose forms they find acceptable. Where ethically and developmentally appropriate -- and we have done this here at ThinkGen -- including adolescents directly in qualitative research reveals insights about independence, stigma, and willingness to adhere to a given modality.
Case Study: HIV Therapeutics
Consider a qualitative conjoint study in the HIV therapeutic space. Patients were asked to evaluate willingness to use existing oral regimens versus innovative administration modalities, including long-acting injectables and once-weekly oral formulations. The results illuminated two dynamics:
Strong preference for reduced frequency—A high percentage of patients leaned toward once-weekly or monthly modalities when framed as reliable and side-effect neutral. Of note, those taking multiple other daily dosed pills, who tended to be older, exhibited a preference to stick with today's QD regimens.
Conditional acceptance of injectables—A segment of patients valued the privacy and reduced pill burden of injections, but concerns about injection-site pain, logistics of clinic visits, and loss of daily “control” were strong counterweights.
By quantifying these trade-offs, researchers could simulate market uptake based upon different TPPs. Importantly, HCPs alone might have overestimated enthusiasm for injections given the concern with adherence; only by including patients did the nuanced picture of conditional (and segmented) acceptance emerge.
The Business Case
Every discontinuation erodes both health outcomes and commercial returns. The cost of non-adherence in chronic conditions is staggering, with studies estimating billions lost annually due to avoidable hospitalizations and complications.
By investing in early, structured primary research on formulation and administration, companies can de-risk development, align with patient and caregiver realities, and compound efficacy into durable market performance.
Conclusion
Efficacy earns regulatory approval. Usability earns routine use. The future of pharmaceutical innovation lies not only in designing better molecules but also in designing formulations and routes of administration that fit the diverse, messy, and very human contexts in which medicines are actually taken.
We care about your data, and we'd use cookies only to improve your experience. By using this website, you accept our Privacy Notice
.svg)